Article Text

Abstract
Background: Lay persons’ judgements of the acceptability of the not uncommon practice of ending the life of a damaged neonate have not been studied.
Methods: A convenience sample of 1635 lay people in France rated how acceptable it would be for a physician to end a neonate’s life—by withholding care, withdrawing care, or active euthanasia—in 54 scenarios in which the neonate was diagnosed either with perinatal asphyxia or a genetic abnormality. The scenarios were all combinations of four factors: three levels of maturity or immaturity, three levels of severity of the health problem, three levels of parents’ preference concerning prolonging care and two levels of decision-making (with or without consulting the other caregivers).
Analyses: Analyses of variance of the participants’ responses were performed to determine the importance of each factor; the interactions among factors, with methods of ending life and with other patient characteristics; and the differences between asphyxia and genetic abnormality. A cluster analysis was performed to look for groups with different patterns of responses.
Results: Lay people assigned most importance to the parents’ request and to the severity of the problem. Except for a small group (12%) always opposed to ending life, they used a simple additive-type rule in integrating the information.
Implications: Most of this sample of French lay people are not categorically for or against ending the life of a damaged neonate, but judge its degree of acceptability by adding up those factors that seem most salient to them.
Statistics from Altmetric.com
Should physicians provide care to all neonates, even those born at the limit of viability or with severe damage, or should they be able to withhold or withdraw care from those neonates at high risk of very bad outcomes?1 2 3 In Europe and North America, official policies, actual practices and the opinions of health professionals and parents provide varied answers.
Legislation and clinical guidelines across Europe4 agree that, in the case of impending death, treatment should be limited and suffering alleviated, even at the risk of hastening death. In the other cases, especially when death is not imminent but the infant’s future is bleak, there is no common position. Active ending of life—active euthanasia—is, however, always prohibited. In the words of France’s Ordre des Médecins, “in no case does a doctor have the right deliberately to provoke death”.5 6
In practice,2 7 8 9 10 11 between 61% and 96% of physicians in different European countries have acknowledged deliberately limiting intensive care to neonates at least once because of incurable conditions, and 46–90% of them have acknowledged limiting it because of the infant’s poor neurological prognosis.7 Withdrawing care, specifically mechanical ventilation, also varied by country (28–90%), and administering drugs to hasten the end of an infant’s life at least once was reported commonly only in The Netherlands (47% of physicians) and France (73%).7
In response to a vignette of a 24-week gestational age infant with a birth weight of 560 g and an Apgar score of 1 at 1 minute,12 most neonataloglists across Europe, except in The Netherlands, indicated they would resuscitate this infant and start intensive care. If told, however, that the infant had developed a severe intraventricular haemorrhage, the percentages of physicians who would limit or end care, with or without parental approval, varied greatly across Europe. In France, where neonatalogists were more aggressive in ending care than elsewhere except in The Netherlands, 3% would continue full intensive care without asking the parents; 11% would try to convince the parents that intensive care should be continued; 15% would accept the parents’ decision about continuing intensive care, whatever it was; 33% would try to convince parents that intensive care should be limited or withdrawn; and 56% would limit or withdraw intensive care without involving the parents in the decision (vs only 1% in Great Britain).12 13
Parents around the world want, to different degrees, to be informed about and participate in decisions about their very low birth weight infants, including about life support.14 15 16 17 In Canada, 64% of parents with premature or term infants agreed that “an attempt should be made to save all infants regardless of birth weight or condition at birth” (in contrast to only 6% of health professionals).14 In France,18 19 20 21 however, parents of critically ill children have been comfortable with allowing physicians to be the predominant decision-makers.
The attitudes of lay people other than parents of hospitalised children have not been described. The aim of the present study was, therefore, to study lay people’s attitudes; to find out which of five factors identified in the literature as important to physicians and parents—the type of health problem (such as, in this case, perinatal asphyxia or a genetic abnormality), the severity of this problem, the gestational age (degree of maturity or prematurity of the infant), the attitude of the parents about prolonging care, and the physician’s consultation or not with the other care-giving personnel—are most salient to them; to see if the type of life-ending intervention (withholding care, withdrawing care, or giving a lethal injection) matters to them; and, moreover, to elucidate the cognitive process by which they form judgements about the acceptability of ending a neonate’s life.
Methods
Participants
The aim was to enrol 250 persons for each of six groups characterised by vignettes depicting one of the two types of illness and one of the three types of life-ending interventions. Accordingly, six teams of researchers, one for each group, approached 2500 adults walking along the main sidewalks of four cities in southern France (Toulouse, Montpellier, Perpignan and Narbonne). After receiving a full explanation of the procedure, 1635 (65%) of them agreed to participate.
Material
The material consisted of 54 cards containing a story of a few lines, a question and a response scale. The stories were composed according to a four within-subject factor design: the child’s gestational age (born at 6 months (“extreme prematurity”), at 7 months, or at 9 months (“term”) gestation) × the child’s health problem (described in the next paragraph) × the attitude of the parents about prolonging care (not known, informed about their children’s health condition and favourable to prolonging care (“that everything be done to keep the baby alive”), informed and unfavourable to prolonging care (“that the life of the baby not be prolonged needlessly”)) × the way the decision was made (individually by the physician or collectively after discussion with the team).
For half the participants, the baby’s health problem was described as asphyxia before or during the delivery with one of three levels of resulting disability: (1) “The consequences will be serious. The infant will have serious learning problems and motor difficulties”; (2) “The consequences will be very serious. The infant will have a mental development of no more than a 3-year-old. He will have no autonomy in, for example, toileting or walking”; or (3) “The consequences will be catastrophic. The infant will remain, all his life, in a vegetative state.” For the other half, the baby’s health problem was described as a genetic disorder with one of three levels of severity: (1) “He suffers from trisomy 21 without any major morphologic anomaly. In spite of obvious mental retardation, the child will be able to be happy and will have a satisfactory quality of life”; (2) “He suffers from trisomy 21 with serious morphologic abnormalities, notably cardiac, which will have very serious repercussions on his future life. In addition to a resulting developmental delay and a very pronounced mental retardation, he will undergo multiple very burdensome surgical interventions”; or (3) “He suffers from trisomy 13, which will have catastrophic repercussions on the quality of his future life. In addition to extremely serious morphological anomalies, notably neurological (microcephaly), the infant will have very delayed development. This genetic anomaly implies death in the very short term.” Other information was held constant: all children were boys, had been delivered 10 days ago, and were currently receiving the best possible care.
At the end of each story, it was stated that the physician acts in one of three ways to end the infant’s life. For one group, the physician decides to “limit care”. For a second group, he decides to “stop care”. For a third group, he decides to give the baby “a lethal injection”. Half of each group of lay participants considered babies with asphyxia, and the other half babies with a genetic abnormality.
The question under each story was “To what degree do you consider that such a decision is acceptable?” The response scale was an 11-point scale with a left-hand anchor of “Not at all acceptable” and a right-hand anchor of “Completely acceptable”. Two examples are given in the appendix. The cards were arranged by chance and in a different order for each participant.
All the participants answered additional questions about age, gender, educational level, religious belief, religious background and attitudes towards the current laws about euthanasia and physician-assisted suicide.
Procedure
The site was either a vacant classroom in the local university or the participant’s private home. Each person was tested individually. The session had two phases. In the familiarisation phase, the experimenter explained what was expected and presented each participant with 27 stories taken randomly from the complete set. The participant read each story out loud, was reminded by the experimenter of the items of information in the story, and then made an acceptability rating by putting a mark on the response scale. After completing the 27 ratings, the participant was allowed to look back at his or her responses and to compare and change them. The purpose was to make the participant as familiar as possible with the test material and the task.22 In the experimental phase, each participant gave ratings for the whole reshuffled set of 54 stories, working at his or her own pace, but was not allowed to look back at and change previous responses. In both phases, the experimenter made certain that each subject, regardless of age or educational level, was able to grasp all the necessary information before making a rating.
The participants took 20–40 minutes to complete both phases. The experimental phase went quickly because they were already familiar with the task and the material. None of them complained about the number of vignettes they were required to evaluate nor about the credibility of the proposed situations. They then completed the questionnaire.
The protocol was approved, as part of a larger study including neonatal nurses and physicians, by the Committee on Ethics of the Hospital of Beziers, France.
Data analysis
There were six groups of participants (two types of illness × three methods of ending life). Their responses (from 0 to 10 on the response scale) were analysed, at the group level, by performing analyses of variance (ANOVA) and by constructing graphs. The design of the two ANOVA (one for asphyxia and the other for genetic disease) was method × gestational age × severity × parents’ attitude × consultation, 3 × 3 × 3 × 3 × 2. Method was a between-subjects factor; the others were within-subject factors. In light of the multiplicity of comparisons, the level of significance was set at 0.001.
A series of complementary ANOVA were conducted that included participant’s age or participant’s gender as a between-subjects factor or that included type of illness and method as two between-subjects factors.
A cluster analysis was conducted on the raw data for all the participants to look for groups of participants with very different patterns of responses from the rest.
Finally, in order to characterise the cognitive rule used for integrating information, two ANOVA with a design of gestational age × severity × attitude × consultation, 3 × 3 × 3 × 2, were conducted (one for asphyxia and one for genetic disease). When people combine pieces of information, they use, unconsciously, integration rules such as addition, multiplication, or averaging.22 The participants whose judgements were used for these analyses were only those who had in fact integrated the information, ie, who had taken the various pieces of information in the vignettes into account when making their judgements. Participants who gave uniformly low or high acceptability ratings had not combined the information—had not used any integration rule—and were, therefore, not included.
Results
The overall mean value of all the ratings was 4.32. The highest mean response, 8.25, was far from the possible maximal answer, 10. There was thus no ceiling effect to complicate the interpretation of the results. We report here only the major findings.
Characteristics of participants
The six groups of researchers were not equally successful in recruiting participants. The actual number of participants in each condition—that is, who judged vignettes depicting one type of health problem and one type of intervention—is shown in table 1.
Number of participants in each condition
The variability in the size of each group did not affect the results.
All participants reported good health. Their characteristics are shown in table 2.
Characteristics of participants by gender
Primary ANOVA
Asphyxia
The method used to end the baby’s life was not significant. All four within-subjects factors, however, had significant effects (see table 3 and fig 1). The less mature the child, the more severe the health problem, the more the parents opposed the needless prolongation of care, and the more collective the decision, the more acceptable did the participants find the life-ending procedure. The attitude of the parents had the most impact, followed by the severity of the health problem.

In the case of asphyxia, the effect on the acceptability judgements (the vertical axis) of (1) attitude of the parents towards continuing care (the three curves), (2) severity of the illness (the horizontal axis), (3) involvement of the team in the decision (the left vs right figures) and (4) gestational age (the three levels of figures).
Effects of within-subject factors
Genetic disease
The method of ending life was significant: active euthanasia (lethal injection) was judged less acceptable (average level 3.48) than withdrawing (4.57) or withholding (4.33) care (p<0.001). All four within-subjects factors also had significant effects (table 3 and fig 2). The less mature the child, the more severe the health problem, the more the parents opposed the prolongation of care, and the more collective the decision, the more acceptable did the participants find the procedure. As in the case of asphyxia, the attitude of the parents had more impact than the other factors, followed by the severity of the health problem.
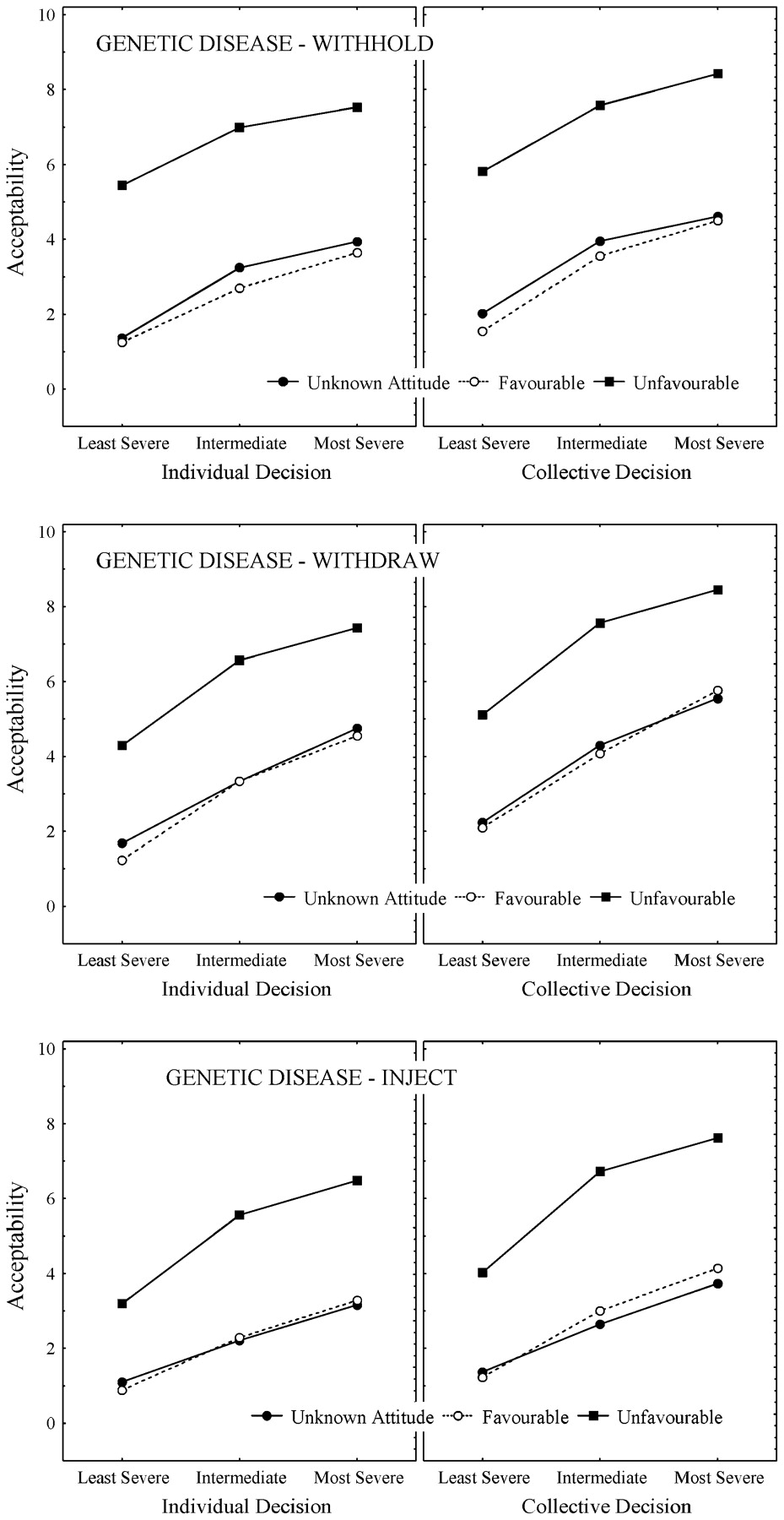
In the case of genetic disease, the effect on the acceptability judgements (the vertical axis) of (1) attitude of the parents towards continuing care (the three curves), (2) severity of the illness (the horizontal axis), (3) involvement of the team in the decision (the left vs right figures) and (4) method of ending life (the three levels of figures).
Complementary ANOVA
Acceptability increased with the age of the participant for infants with both asphyxia (average of 4.52 among older adults vs 3.89 among very young adults) and genetic disease (5.41 vs 4.13). Neither gender nor any interaction involving gender had a significant effect. The overall acceptability was lower for the use of active euthanasia for genetic disease (3.48) than in all other cases (4.48).
Cluster analysis
The cluster analysis identified a two-cluster solution. In light of the patterns of their members’ responses to the vignettes, the first cluster (N = 202, 12%) was called “always unacceptable”, the second (N = 1433, 88%) “depending on circumstances”. The mean acceptability ratings were 1.01 and 4.60, respectively (p<0.001). The two clusters differed significantly in only two characteristics: 68% of the first cluster versus 87% of the second favoured modifying the laws concerning euthanasia and medically assisted suicide, and 64% of the first versus 48% of the second indicated a belief in God.
Integration rules
The complementary ANOVA conducted on the data from the asphyxia vignettes of the participants in the “depending on circumstances” cluster found that all the main effects were significant and that no interaction involving one or several of the four factors was significant. The pattern of results is portrayed in fig 1. All curves are ascending, showing that acceptability increases as the disease becomes more severe. The curves corresponding to parents’ unfavourable attitudes to prolonging care are clearly higher than those representing favourable attitudes, and those for the scenarios in which the parents’ attitude towards prolonging care was not known are almost superimposed on the favourable curves. The curves on the right, representing involvement of the team, are higher than those on the left. The curves in the bottom panels (gestational age 9 months) are only slightly lower than those in the top panels, reflecting the quite small effect on acceptability of gestational age. All curves are roughly parallel, which demonstrates the additivity (the non-interactivity) of the four effects.
For genetic disease, in the “depending on circumstances” cluster all the main effects were again significant, but the bilinear components of the three two-way interactions involving severity, parents’ attitude and consultation with the team were also significant. The diverging pattern, which is clearly visible in the bottom panels in fig 2, attests to this slight interactivity of effects.
The difference between the “depending on circumstances” and the “always unacceptable” clusters is portrayed in fig 3, where the curves for the “always unacceptable” cluster are low, almost flat, and at only slightly different levels, attesting to the lack of effect of the primary factors of parents’ attitude and severity of the disease.

{kind=link}
{kind=link}
{kind=link}
For the two observed clusters of participants, “always unacceptable” (left) and “depends on circumstances” (right), the level of acceptability (vertical axis) in relation to attitude of the parents towards continuing care (the three curves) and severity of the illness (the horizontal axis).
Discussion
The present study examined how lay persons judged the acceptability of three methods of ending the life of a damaged newborn, ie, of a neonate who, because of either perinatal asphyxia or genetic disease, was destined to have more or less severe disability. They judged active euthanasia (lethal injection) as less acceptable than withdrawing care and withholding care, but only to a small degree and only in the case of genetic disease, not in the case of perinatal asphyxia. These results are consistent with previous findings that for lay persons, active euthanasia of very sick adults is not much less acceptable than passive procedures (eg, withholding care).23
All the information factors in the scenarios—the baby’s gestational age, the severity of the baby’s health problem, the attitude of the baby’s parents about prolonging care and the decision of the doctor to consult or not with the other caregivers—had significant effects on judgements of acceptability, but the attitude of the parents about prolonging care was by far the more important factor. For asphyxia as well as for genetic disease, this factor explained about three-quarters of the variance of the acceptability judgements. These results are consistent with the desire of parents to be involved in the decision-making process;15 17 20 with the importance of patient request in ending adults’ lives;24 25 and, moreover, with the finding that, when an adult patient is not in a position to make a request, the family’s attitude towards ending life becomes the determining factor.26 In addition, the current study discovered that, when parents’ attitudes were not known, people’s ratings of the acceptability of ending a baby’s life were as low as when the parents wanted everything done, ie, the default was to prolong care.
The second most important factor was the severity of the baby’s health problem, which is consistent with the finding that suffering ranks second in importance behind patient requests in judging the acceptability of ending adults’ lives.23 24 The doctor’s consulting or not with the team and the baby’s gestational age had only minor effects.
The lay participants could be separated into clusters on the basis of their attitudes towards ending these babies’ lives. One small cluster (12%) always considered life-ending procedures as unacceptable. Similarly, in other studies, small numbers of participants declared that stopping life-prolonging care of adults26 or giving a teenager an abortion27 is unacceptable irrespective of the circumstances. The other cluster (88%)—less likely to believe in God than the first, but not differing from it in age or gender—took all the information into account, to a variable extent, in judging acceptability. The people in this cluster were still reluctant to condone ending life if the parents were opposed or if their opinions were unknown, giving an overall mean acceptability of only 4.60 (on the scale of 0 to 10). Acceptability was greater than 8 only if the parents were unfavourable to prolonged care, the consequences of the disease were very severe, the decision was taken collectively and the baby’s gestational age was less than 9 months.
The cognitive rule used by most lay participants to integrate the different pieces of information when the neonate had perinatal asphyxia was a simple additive-type rule, with all factors contributing independently to the judgement:
Acceptability = gestational age + severity + parents’ attitude + consultation
People also use an additive rule to judge the acceptability of ending the lives of adults.24 25 26 When, however, the babies had a genetic disease, the cognitive rule was more complex, involving several interactions; that is, the effect of a factor depended, to some extent, on the levels of the other factors. Nonetheless, these interactions were always weak, so that even for genetic disease, the equation above remains a good approximation of the process of integrating the information.
Limitations
The study has limitations. First, the sample, although quite large, is a convenience sample of lay people in southern France. In addition, we do not know how they differed from the 35% who were approached by researchers but declined to participate. The results must, therefore, be generalised with care to the French as a whole and to people in other countries.
Second, the participants made decisions about vignettes, not about real patients. It may be easier to agree to ending the life of a paper than a real patient. Nonetheless, the use of vignettes is common, is necessary in order to manipulate only a select number of variables, and has been validated in other contexts.28
Third, the necessary restriction of variables within the vignettes to only a few, in this case to five factors, means that other potentially important factors could not be included. It was thus crucial to choose those factors already demonstrated to be important.
Fourth, uncertainty about the outcomes of individual patients is usually greater than presented in the vignettes. As this uncertainty increases, we would expect parents to be less comfortable with definite actions, especially with ending their babies’ lives. To enable participants to focus on the study factors, we presented cases whose outcomes would, in fact, be relatively well known and clear cut, even if less certain than suggested in the vignettes. It would be useful in the future to study the impact of different degrees of uncertainty.
Fifth, the participants made judgements about decisions that had already been made, ie, the doctors had already decided to end the babies’ lives. Psychologically, whether a life-ending action should be undertaken is a very different question than to what extent such an act, already done or at least already decided, should be condoned. The latter is an easier question; less costly in time and in cognitive and emotional stress; and more natural to participants who would regularly, in real life, give opinions about the actions of others. Moreover, it would have seemed artificial to French lay people to be asked to make decisions that only the neonatologists and parents are in a position to make.
Sixth, even though French participants would assume that the neonatology team would keep all babies as comfortable as possible and were told this by the experimenters before both phases of the study, some of them may have worried during the study that babies whose lives were ended would undergo unacceptable suffering and may, therefore, have been less willing to condone ending their lives. We plan to examine this issue in a future study.
Conclusions
In judging the acceptability of ending the lives of newborns destined to have major disabilities, the French lay persons in our study appeared to realise that the decision to end a life is more important than the method chosen to do it. A few of them were, like French law, absolutist in condemning all life-ending acts. The vast majority, however, judged acceptability as a function of the circumstances. They asserted that ending the baby’s life was increasingly acceptable as the factors combined to favour it. Each factor contributed, in an additive if unequal fashion, to overall acceptability. In contrast, in legislation on euthanasia and physician-assisted suicide for adults in The Netherlands and elsewhere, ending life is either acceptable or it is not, ie, it requires a set of criteria to be fulfilled before it is legitimate to end a patient’s life.29 30 31 People appear to be more compensatory and less rigid than the law, whether it prohibits or permits life-ending actions.
The most important factor for our participants in judging the acceptability of ending a damaged neonate’s life was the parents’ desire concerning the continuation of treatment. This was more important than the severity of the disease, ie, than the projected burden of disability and suffering for the baby and for the family. If, as already noted in this paper, French neonatologists are willing to act without consulting parents7 12 and French parents defer to neonatologists in decision-making about their premature infants,20 21 the French lay people, like American parents,20 21 asserted the primacy of autonomy over beneficence and non-malfeasance in neonatal decision-making.
Acknowledgments
The authors would like to thank Charles Vanraet for contributing the data he collected for his undergraduate thesis.
APPENDIX
Two examples of vignettes
Baby Thomas has been hospitalised since his birth (10 days) in the neonatology service at the Hospital Claude Bernard. He was born more or less at term. Before or during the delivery, he had a period of asphyxia. The consequences of this will be serious. The infant will have serious learning problems and motor difficulties. The parents are well informed about the true condition of their infant including everything this condition implies. They express clearly the desire that everything be done to keep the baby alive. Doctor Bernard decides, by himself, to give Thomas a lethal injection.
Baby Manuel has been hospitalised since his birth (10 days) in the neonatology service at the Hospital Ambroise Paré. He was born at 6 months’ gestation, that is, extremely premature. He has trisomy 13, which will have catastrophic repercussions on the quality of his future life. In addition to extremely serious morphological anomalies, notably neurological (microcephaly), the infant will have very delayed development. This genetic anomaly implies death in a very short term. The parents are well informed about the true condition of their infant, including everything this condition implies. They express clearly the desire that the life of the baby not be prolonged needlessly (no extraordinary treatment). Doctor Gyclor decides, after several long discussions with the members of his team (nurses, psychologist and other doctors), to stop the care given until now to Manuel.
To what degree do you think that such a decision is acceptable?
Not at all acceptable o----o----o----o----o----o----o----o----o----o----o Completely acceptable
REFERENCES
Footnotes
Competing interests None.
Ethics approval The protocol was approved, as part of a larger study including neonatal nurses and physicians, by the Committee on Ethics of the Hospital of Beziers, France.
Provenance and peer review Not commissioned; externally peer reviewed.
Other content recommended for you
- The acceptability among young Hindus and Muslims of actively ending the lives of newborns with genetic defects
- A case for justified non-voluntary active euthanasia: exploring the ethics of the Groningen Protocol
- End of life decision-making in neonatal care
- Letting babies die
- Magnetic resonance spectroscopy in preterm infants: association with neurodevelopmental outcomes
- Development and validation of a model to predict mortality risk among extremely preterm infants during the early postnatal period: a multicentre prospective cohort study
- The acceptability of ending a patient’s life
- Passive euthanasia
- Randomised controlled study of oral erythromycin for treatment of gastrointestinal dysmotility in preterm infants
- Euthanasia: above ground, below ground